DIGITAL
RADIOGRAPHY
______________
Author: Dr. Boban Fidanoski, DMD
History of Digital Radiography
On November 8-th 1895, a Bavarian physicist Wilhelm
Conrad Roentgen was intrigued by glowing cathode tubes and decided to see
what they could do. He found that the rays they emitted could pass through body
parts, such as his hand, the bones beneath the skin became clearly visible on
the screen. Because he didn't know exactly what was causing this phenomenon, he
labeled the rays "X", which is the mathematical symbol for anything
that is unknown. The revolution has just begun. Less than two weeks after this important discovery, Dr.
Otto Walkhoff developed the first original dental “roentgenogram” from a
portion of a glass imaging plate. The image required 25 minutes of exposure.
Radiography and Dentistry has just started a very good friendship.
The dawn of the digital era in dental radiography came in 1987 when the first digital radiography system called RadioVisioGraphy, was launched in Europe by the French company Trophy Radiologie. The inventor of this system was Dr. Francis Mouyen. He invented a way to employ fiber optics to narrow down a large x-ray image onto a smaller size that could be sensed by a Charge Coupled Device (CCD) image sensor chip. Once the X-Ray imaging chip specifications were finalized, Trophy Radiologie contracted Fairchild CCD Imaging Company in Silicon Valley, California, USA to develop the actual CCD imaging chips. At Fairchild, a young Finnish physicist and CCD image sensor design engineer named Paul Suni helped create the enabling CCD image sensor technology that was needed to make the RVG digital radiography system a reality. The new technology was ready to expand. Two decades after, today’s digital radiographic systems have developed a great superiority and have many benefits.
Fundamental Principles of Digital Radiography
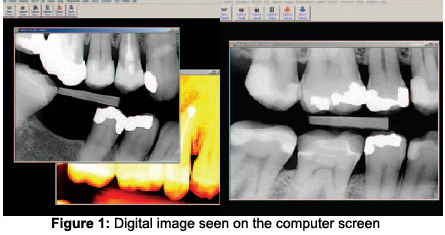
Digital radiography refers to a method of capturing a radiographic image using a sensor, breaking it into an electronic pieces, and presenting and storing the image using a computer. In stead of having an analog radiographic image on a film, in digital imaging the sensor is used to receive the analog information and through analog-to-digital converter (ADC) to convert it to a digital image that is an array of picture elements called pixels, with discrete gray values for each one. Special software is used to store and manipulate the digital image in the computer. The image is displayed within seconds or minutes on the computer screen in front of the clinician and the patient/client.
Radiation Exposure and Biologic Effects of Digital Radiation to Clients and Operators
Digital radiography requires less x-radiation than conventional radiography. Due to their larger sensitivity sensors provide an equivalent clinical image with about 70% less exposure to radiation than D-speed conventional film, and with the latest advances in F-speed film conventional technology, digital imaging still provides an equivalent image with about 20% less radiation. With less radiation exposure, the absorbed dose to the patient/client is significantly lower.
Advantages of Digital Radiography
One of the most valued advantages is Superior gray-scale resolution of 256 colours of gray in comparison with 16 to 25 shades of gray on a conventional film. This property allows facilitated contrast and density manipulation in order to enhance features or details of diagnostic importance, without additional exposure for the patient/client to take another radiographic image. Colourization and enlargement of the images are great features of the digital radiographic software, as well as manipulation with contrast, sharpness, image orientation and pseudocolour alteration. Taking two images on the same area but in the different time and reversing their gray scale using the software will be useful for determination and analysis of patterns that may be characteristic of a particular disease or condition (see Subtraction Radiography, page 9). Previously explained reduced exposure to x-radiation is also a great advantage of digital radiography. Decreased processing time that digital radiography offers is of a great financial and professional value to any clinician. Only seconds or minutes take apart taking the digital image and viewing it on the computer screen. Extra saved time can be used for other important daily duties of a dental professional. Storage of radiographs into the small hard drive of the computer is a great space saver in comparison with extra sheet of radiographs in each patient’s/client’s folder in the file shelves. Digital images are easily transmitted to other offices. Laptops, removable discs and CDs allow the systems to be easily moved. After initial setup cost, everything else on a long run is financial saver: digital radiography eliminates the need for purchasing conventional films, costly processing equipment and solutions. Darkroom is no longer needed, and it can be used for other more useful purposes in the dental office. Converting into the digital radiography will distinguish the dental office as environment friendly because no disposal hazards of processing chemicals, silver salts in film emulsion and lead foil sheets will exist.
Extreme importance of Digital Radiography in Implantology
When accomplishing implant placement, using conventional radiography is a major inconvenience, as the entire aseptic procedure is disrupted and time is wasted while the clinician awaits the development of the films several times during the implant placement procedure.
Advantage of Digital Radiography during the Endodontic treatment
The digital image is available on the computer screen within a few seconds. As a result, digital radiographic systems are efficient aids in an endodontic procedure, in which a second image easily can be made from a slightly different angle without removing the sensor out of patient’s/client’s mouth—for example, to make the second root canal better visible—with the sensor still in the same position, but with different angulation.
Disadvantages of Digital Radiography
Initial cost for purchase and set up of the equipment as well as the cost for personnel’s training how to properly use the equipment is a disadvantage of the digital imaging systems. Sensors are the weak part of the system due to their relative rigidity and thickness ( approximately 5 millimetres) that could produce uncomfort or pharyngeal reflex in patients/clients. The viewable surface area is smaller than the
total size of the sensor and sometimes sensors are not universal and interchangeable between different
systems. Digital sensors can’t withstand heat sterilization, therefore they require complete coverage with disposable plastic sleeves (see Infection Control, page 11). Digital radiographs have legal issues because of their potential for fraudulent use (see Legal issues in Digital Radiography, page 12)
Equipment
The essential components of digital imaging include:
I. X-radiation source: most digital systems use conventional
dental units as x-radiation source due to its compatibility.
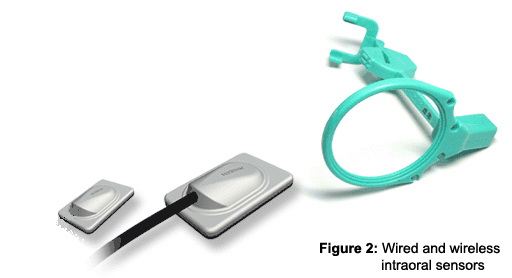
II. Intraoral Sensor: is a small detector that is placed intraorally and
used to capture the radiographic image and send to the computer for future
processing. Sensors are similar in dimensions like conventional films and may
be either wired with 8 to 35 feet fiberoptic cable for transmittion of
generated image to the computer or wireless. Intraoral sensor is composed of a
silicone chip and a layer that surrounds it. A layer above the sensor chip is the scintillator (material that emits light when particles traverse
it), which converts x-ray energy into
light and directs it towards the top layer of the chip that is more sensitive
to light than x-rays. Top layer of the chip then releases electrons that form
the image and send them onto the well in the lower portion of the chip. The
energy in each well is then read and digitized with an A/D (analog to digital) converter
during the read-out process.
Currently three types of sensor technologies
exist:
1. Charge-coupled device
(CCD)
This is one of the
most common image receptors in digital radiography, an old technology since
1960’s and is used in many other devices like fax machines, video cameras, microscopes
and telescopes. The CCD is a sensitive to x-rays or light, it is a solid-state
detector that contains a silicone chip with an electronic circuit embedded in.
2. Complementary metal oxide semiconductor/active pixel sensor (CMOS/APS)
The silicone chip for this type of sensor is less expensive to produce,
offers greater durability and 25% greater resolution than charge-coupled device
(CCD) sensor.
3. Charge injection
device (CID)
This type of sensor
doesn’t require computer for image processing. The CID sensor uses the same
docking platform with intraoral camera, and within seconds directly produces
digital image that can be seen on the monitor. Later on, this image can be
saved in the computer or on a video disc recorder.
Difference between wired and
wireless sensors: Wireless
sensors are thicker than wired sensors, and the battery life is an
important cost consideration when comparing systems. The image quality is
not affected by the wireless transmission. Wireless systems are typically
1.5 x as expensive as their wired counter part. Another concern is losing
or dropping of the sensor.
III. Computer: is used to digitize process and store
informations received from the sensor in 0.5 to 120 seconds and then present
the image on the computer monitor. As previously mentioned, this speed is very
useful in endodontic and implant surgical procedures. The image may be stored
permanently on the computers hard drive, printed on a hard copy or transmitted
electronically to insurance companies or referring dental specialists.
Techniques for exposing,
processing and mounting digital radiographs
Currently, there are two types
of digital radiography systems available: direct and indirect:
I. Direct
Digital Imaging
X-ray photons
that originate from the conventional radiographic unit come in contact with
the intraoral sensor and cause electrons to be released from the silicone chip
and produce latent image. Electrons travel to the computer unit where are converted
into pixel arrangement that can be visually seen on the computer monitor. A
pixel is digital equivalent of a silver crystal used in conventional radiography.
For example, CCD sensor can produce 640x480 individual pixels in size. Each
pixel is represented numerically in the computer by levels of colour of gray
and varies from 0 to 255, which creates 256 shades of gray, referred to as a
pixel’s gray-scale resolution. Zero on this scale means that the maximum radiation is measured, which
corresponds to black in the radiographic image (radiolucency), and 255 represents
no radiation at all, or complete radiopacity (white).The number of possible gray-scale
combinations per pixel is known as bit-depth image. Digital image with
256 pixel resolution contains 8 bit-depth_image.
II. Indirect Digital Imaging
1. Scanning of traditional radiographs
With this
method, an existing conventional radiograph is digitized using CCD camera, which
scans, converts image from analog to a digital form and then displays it on
the computer monitor. This is an extremely slow procedure since it occupies
the time needed first for production of conventional radiograph and then extra
time for production of digital image.
2. Storage Phosphor Imaging or Photostimulable Phosphor Plate (PSP)
This method
employs reusable imaging plate coated with phosphors instead of sensor. After
radiation exposure and capture of the image on the plate, a high-speed scanner
is used to convert information into electronic image. Time needed for processing
the image from the plate into the computer is between 1.5 and 5.5 minutes. After
its transmittion into the computer, the radiographic image is cleared from the
plate by exposure to viewbox light for several minutes and is ready for reuse.
Indirect digital imaging typically refers to Photostimulable Phosphor Plate
(PSP) technology which has been around since 1981, and is the basis of nearly
all hospital digital radiography systems. Although theoretically plates
can be used indefinitely, in practice plates are replaced approximately every 3 months or 50 exposures.
Subtraction Radiography
Subtraction in digital radiology is another image enhancement method with purpose to produce two radiographs of the same area in the mouth at the different time intervals. The first image can be subtracted from the second one to identify changes that may have occurred during a certain time period. Minimal changes in loss or gain of hard tissue can be detected using this technique, otherwise undetectable by visual examination and traditional radiography. A main requirement for subtraction digital radiography is an identical or almost identical image projection at these different time periods. This procedure of image registration (alignment of the two views) also requires correct exposure and processing techniques.
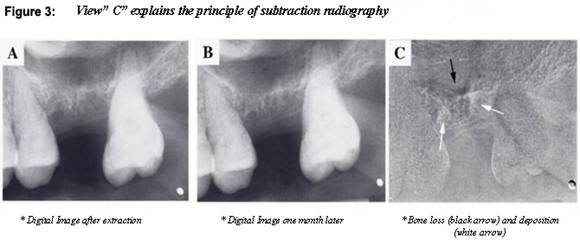
The most recent method used to assure proper alignment is to place the patient in a cephalostat (head stabilizing device) with a fixed x-ray source and securing the film to the teeth with silicone impression material to help produce images with reproduced geometry. This technique triggered a most recent development of tools that can recognize anatomic features, rotate, align, and scale two images for automatic image registration.
Step-by step procedure for the use of digital radiography system
1. Proper infection control of the intraoral sensor
2. Placement of the sensor in the patient’s/client’s mouth on a conventional film holder. Paralleling technique is the preferred exposure method.
3. Radiation exposure of the sensor with conventional radiographic unit.
4. Digitalized conversion of the analog image into the computer, directly through fiberoptic cable or wireless or indirectly through scanning of the conventional radiograph or phosphor plate and then transfer into the computer and its conversion into the digital image.
5. Display of the digital image
on the computer monitor for diagnostic purposes of the current procedure.
Infection control in Digital Radiography
Digital sensor is reusable device but can not stand the heat during the sterilization due to its constitution. Therefore, for infection purposes the sensor must be covered with a disposable barrier. However if it becomes directly contaminated there is no way of sterilizing and the sensor should be discarded regardless of the expense. Use of a barrier does not always protect from contamination. To minimize the potential for device-associated infections, after removing the barrier, the device should be cleaned and disinfected with an EPA (Environment Protection Agency)-registered hospital disinfectant (intermediate-level) after each patient.
Quality Assurance and Diagnostically Acceptable Radiographs in Digital Radiography
The majority of the studies conclude that the diagnostic quality of digital images certainly is adequate; digital images perform at least as well as conventional radiographs and sometimes even better. The resulting image from the system is the true test of its capability and can be measured in several ways. Two of the more common ways are spatial resolution and gray scale resolution. Spatial resolution is the capacity to detect small details, and usually measured in line pair per mm (LP/mm). Most conventional E-speed films have resolution of 20 line pair per millimetre (LP/mm) whereas with digital images the resolution ranges from 7 to 10 LP/mm. On the other hand, the resolution expressed in gray scale is more than adequate. Newer sensor systems capture the images at bit depths of 12 to 16, instead of the lower 8 bit (256 colours of gray) depth that was common in the past. The higher bit depth will improve image quality under different exposure conditions. Although the human eye can only detect 16 different gray scales, the computer can use the information to provide a better image to the display. Numerous studies have demonstrated that direct digital radiographs are equal in diagnostic quality to conventional radiographs.
Legal issues in Digital Radiography
Radiographic records also provide valuable information about whether treatment was justified. Digital dental radiographs can be altered to show an apparent need for treatment that is not real or to show completed treatment that has not actually been performed. Some available digital radiographic softwares will not permit image alteration or will add an error sign if an image is altered. However, images that have an error sign on them can be imported into an image-editing software program in which the error sign can be removed. An electronic file also has several time stamps that indicate the creation date and time of the file, the last time it was accessed, and if and when the file may have been changed. Of course, it is possible to fool the computer’s time setting, and alter the image. Then the new altered image could be saved into the computer instead of the old one, submitted on new film or reprinted on duplicating film. The altered images can be used to charge insurance companies for treatment that was not actually performed.

Future of Digital Radiography in three dimensions
Three-dimensional reconstruction and rendering of radiographic image data has been introduced recently in the form of Cone Beam Computerized Tomography (CT) and Local CT. Both cone beam and local CT have imaging geometry comparable with that of conventional CT, but offer a higher resolution with a much lower radiation dose to the patient. The image appeared on the computer screen in three-dimensional.
Summary: Digital Radiography is a powerful tool for dental practice
Digital dental radiography, in practice of dental professional is a powerful tool. Some of the most important benefits this technology offers include patient education, time efficiency, reduced exposure to radiation (for the patient and practitioner), and environmentally friendly set up. The initial appointment is usually the most critical time for patient assessment, not only from the data collection standpoint (in preparation for diagnosis), but also patient education. Use of digital radiography saves a hygienist time, when compared with the traditional radiography, which can be utilized for building a report with the patient, educating patients on dental health, and proper assessment and diagnosis.
________________________________________________________________________________
Bibliography:
Haring, J.I., Howerton, L.J. (2006): Dental Radiography, Principles and Techniques, 3-rd Ed., USA.
Kantor, M.L., DDS, MPH (October 2005): Dental Digital Radiography-More than a fad, less than a revolution-Journal of American Dental Association (JADA) Vol.136, USA
Van der Stelt, PF, DDS., PhD (October 2005): Filmless Imaging, The uses of Digital Radiography in Dental Practice, Journal of American Dental Association (JADA), Vol. 136
Christensen, G.J., DDS, MSD, PhD (October 2004): Why switch to Digital Radiography? Journal of American Dental Association (JADA), Vol. 135, USA.
Florman, M., DDS (2005): The Practice of Digital Dental Radiography; The Academy of Dental Therapeutics and Stomatology, Chesterland, Ohio, USA.
Cybula-Tahmazian, K. RDH: Dental Diagnosis with Digital Radiography http://www.umdnj.edu/idsweb/tech_reviews/Kathy/ - University of Medicine and Dentistry of New Jersey, USA.
Tsang, A. D.M.D et al. (September 1999): Potential for Fraudulent use of Digital Radiography, Journal of American Dental Association (JADA) Vol.130, USA.
Wenzel, A. (June, 2002): Two Decades of Computerized Information Technologies in Dental Radiography, Journal of Dental Research (JDR), Denmark
Brennan, J. (2002): An Introduction to Digital Radiography in Dentistry-Journal of Orthodontics, Vol.29, United Kingdom.
Image sources:
Figure
1: Florman, M. DDS (2005): The Practice of digital dental radiography;
The Academy of Dental therapeutics and Stomatology Chesterland, Ohio, USA
Figure 2: Vatech web site: http://www.atx.com.au -Australia
Figure 3: Cybula-Tahmazian, K. RDH: Dental Diagnosis with Digital Radiography http://www.umdnj.edu/idsweb/tech_reviews/Kathy/ - University of Medicine and Dentistry of New Jersey, USA.
Figure 4: Tsang, A. DMD et al. (September 1999): Potential for Fraudulent use of Digital Radiography, Journal of American Dental Association (JADA) Vol.130, USA
|
|
 |
|
