Live Comprehensive
Case Study
______________
Author: Boban Fidanoski
Dental Hygiene Program
Group A - No. 2336
Canadian College of Dental Health

Dental Hygiene Principles III Assignment
Submitted to: Bernadette Mackay, RDH
January 11-th, 2008
Assessment
Client's Personal Information
Client is healthy 57 years old female, temporary visitor to Canada for summer vacation. She temporarily resides in Mississauga, ON. She is native of Republic of Macedonia, a two million inhabitants country in South-East Europe. She lives in the capital city of Skopje, that has approximatelly one million if inhabitants, she is married, has 5 years till retirement, enjoys her two dogs and her occasional travel to distant countries. Client doesn’t smoke or drink alcohol.
Language as a barrier to Dental Hygiene Care
Client has minimal knowledge in English language. As most of the tourists, she is able to communicate in English concerning travel issues and basic life situations, but she is not able to communicate on the dental level with her clinician. She speaks perfectly her native Macedonian language, as well as Serbian, Bulgarian and Croatian language. She has minimal knowledge of French, on the same level like English.
Her language skills are the biggest barrier to her professional dental hygiene care, so in English speaking countries like Canada she would have problems to access her dental hygiene care if there are no clinicians who know Macedonian present in the area where she temporarily resides.
Clinician she has gone to, myself, knows Macedonian language, so this barrier was smoothly removed, although in a Dental hygiene college clinical settings where the work of a student is closely observed by instructors, issue has developed that in this kind of situation student and client will communicate in Macedonian, but instructors will not be able to supervise this communication in regards of students ability to translate consent forms, or to deliver Oral Hygiene Instructions, so everything was left to instructors confidence in student’s work.
This case gave me an idea to propose to our governing body to have a list of Dental Hygienists who speak different languages so the visitors of Canada if they want to access Dental Hygiene Care but are unable to communicate in English they could have some reference where they could find a RDH who speaks their native languageProgress notes and Record of Care
Client visited our student clinic six times in order her dental hygiene care to be completed. In a nutshell, her first three visits were assessment, noting that first visit was during the assessment days and it was only an hour long. Here last three visits were pertinent to the implementation and evaluation of my Dental Hygiene plan, like OHI, periodontal debridement, and evaluation. Her first visit was on June 06-th 2007 and the last one was on July the 18-th, 2007.


Medical and Dental History
Client’s family physician Dr.Stojkovski and dentist Dr.Velkoski, both originating from Macedonia.
Medical History has not revealed any concerns. Her last visit to a physician was in May/2007 and last physical examination a month before. Client is aware of her bone mineral density. No allergies were present.
Vital signs were within normal limits all five visits:
Blood pressure measurements: systolic: highest: 126, lowest: 115
diastolic: highest: 82, lowest: 75
Pulse: highest: 82, lowest: 75
Respiration rate: 16
Dental history has revealed a lot of informations beneficial for her ongoing process of dental hygiene care:
- Clients last dental cleaning was done a year ago, in March 2007
- FMS was taken 3 years ago in 2004, one PA was taken in April/2007
- Client’s gums bleed occasionally while brushing, especially in quadrant 2.
- She has noticed loose teeth among lower incisors
- Food catches between and underneath her dental bridge present in quadrant 1.
- Client doesn’t floss, brushes her teeth twice per day, and cleanses her tongue occasionally
- She experiences clicking in her left portion of TMJ
- Occasionally she grinds and clenches her teeth
Pharmaceutical Record
Client takes ROVAMYCINE on a regular basis for the period of last six months. Client noted that she is aware that she has periodontal disease and in Macedonia she sees her periodontist on a regular basis, and as adjunct to NSPT Macedonian dentists still recommend use of full blown antibiotics like Rovamycin 500 mg. tid to help destroy as many as possible pathogenic bacteria that resides in periodontal pocket.
ROVAMYCINE in Canada is known as SPIROMYCIN, and it use in periodontal therapy was discontinued at the end of 90’s.
Rovamycin is macrolide antibiotic produced by Streptomyces ambofaciens. The drug is effective against gram-positive aerobic pathogens, N. gonorrhoeae, and staphylococci. It is used to treat infections caused by bacteria and Toxoplasma gondii.
Antibiotics have been widely used in treatment of periodontal diseases due to their ability to accumulate in gingival crevicular fluid (GCF) and act as a depot medication against present pathogenic bacteria. In doses of 200 or 100 mg/day they are known to act as bacteroistats against major players in Periodontal disease like Prevotella intermedia, Porphyromonas gingivalis, Bacteroides forsytis and Actinobacillus actinomicetemcomitans. But traditional antimicrobial treatments present with three major limitations:
- Total bacterial elimination is impossible, since the ever present oral flora quickly repopulates with minutes of the removal, even in cases of pocket sterilization
- Antimicrobial treatment does not address the “host-response” aspect of the disease and does not affect the activity of MMPs, which are the end products.
- There is a remarkable possibility of development of bacterial resistance to tetracyclines after their long term use in regular antimicrobial doses ( 250 mg /day for 2-7 years)
Studies up do date has shown that standard antibiotic therapy of 200 to 300 mg is not effective due to immediate repopulation of bacteria flora in oral cavity and increased chance for resistance. Since the host response is the main issue in destruction of periodontal tissue in periodontal disease, the most effective antimicrobial approach was found to be an administration of subantimicrobial dose of Doxycycline of 20 mg. bid, for a period not shorter than three months that help to suppress host response and decrease even more pocket depths after SRP, but has no effects on present bacterial flora thus removing the possibility of development of resistance to antimicrobials.
Consent Forms
Introductory letter by our program director and written consent form were carefully translated and explained to the client in Macedonian language. Client chose the options of fluoride treatment, application of sealants or taking radiographs if necessary and signed the consent form thus giving us green light to continue with dental hygiene process of care. Client also consents to be a case of my live comprehensive study.
Extraoral examination has revealed:
- Slight unilateral dislocation of the left portion of TMJ with shifting o the mandible towards right on opening.
- Brown, round macule present on the right side of the cheek with raised portion towards up, with diameter of 12 mm.
Intraoral examination has revealed:
- Fordyce granules present on upper lip and in the area of left commisures.
- Slight white coating on the tongue
- Bilateral edentulous area in mandible
Gingival Assessment
Generally, colour of gingiva is pink-red, margins are flat, papillae are blunt, consistency is soft and spongy and flabby in edentulous areas. Texture is stippled in anteror segments of maxillary and mandibular arch and smooth in posterior segments.
Locally, gingiva is purple at 27; margins are recessed at 26L and 27L and rolled at 23L and 24L.
Currently there is no present sensitivity on any stimuli.
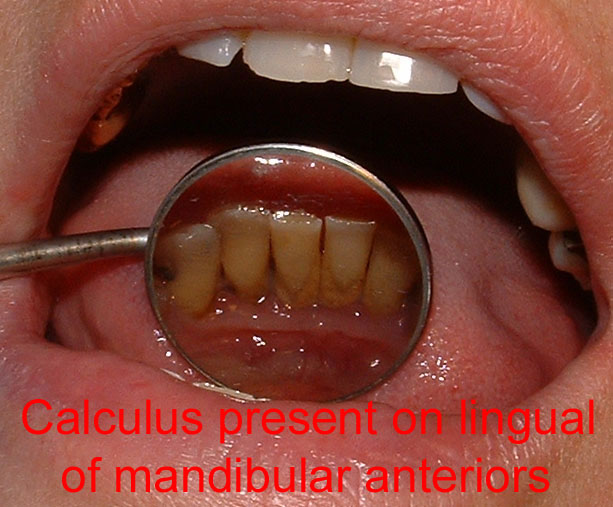
Calculus detection and client’s classification
Upon thorough exploring, moderate to advance accumulation of supra and subgingival soft and hard deposits was found. Client was classified as “C” with a possibility after complete assessment she could be a “D”
Plaque index
Visible accumulation of plaque along gingival margins was found in maxillary posterior sextants and in mandibular anterior sextants that was expected since client doesn’t floss neither uses any interproximal cleaning aids.
Plaque index by Silness and Loe was performed. Score was 1.4, rating: fair.
Radiographic assessment
A Full mouth series of radiographs was ordered by attending dentist in our student clinic. 15 PA’s and 4 Bitewings were taken. FMS was duplicated for client’s future references.
Obstacles while taking radiographs
After initial evaluation I was asked to retake 5 PA’s. My biggest obstacle in taking these radiographs was presence of edentulous areas in mandible. Client has a lower partial denture, but she stated she has left the denture at home, so I wasn’t able to use the denture to bite and stabilize the film. Now, in this situation, without the denture client wasn’t able to bite while I was taking posterior PA’s and bitewings. I was suggested by the dentist and got help by my clinic’s supervisor to use cotton rolls as space filler, so client could bite on cotton rolls. This was a first time experience for me, therefore I had to do 5 retakes.
Although I was present and working in a learning facility and for teaching purposes it was beneficial for me to take FMS, my opinion is that taking 4 bitewings wasn’t beneficial for the client because it didn’t show anything more that PA’s were showing..
Odontogram
Hard tissue exam has revealed:
- Teeth not present: 16, 8, 22, 24, 28, 34, 35, 36, 37, 38, 45, 46, 47, 48
- Gold bridge with buccal composite facets present in quadrant 1: abutments 3 and 17, potics:14,15 and 16
- Cantilever bridge present in quadrant 2: abutments 23 and 25, pontic 22.
- Remnants of a root present in 21 area

Referral letter and its declination by client
Referral letter was decided to be issued by attending dentist, in regards of the remnants of the root present at 21 area. Client chose to decline the letter with explanation that her dentist in Macedonia is well informed about her oral status and appropriate measures are already planned to be taken when she comes back from trip to Canada.
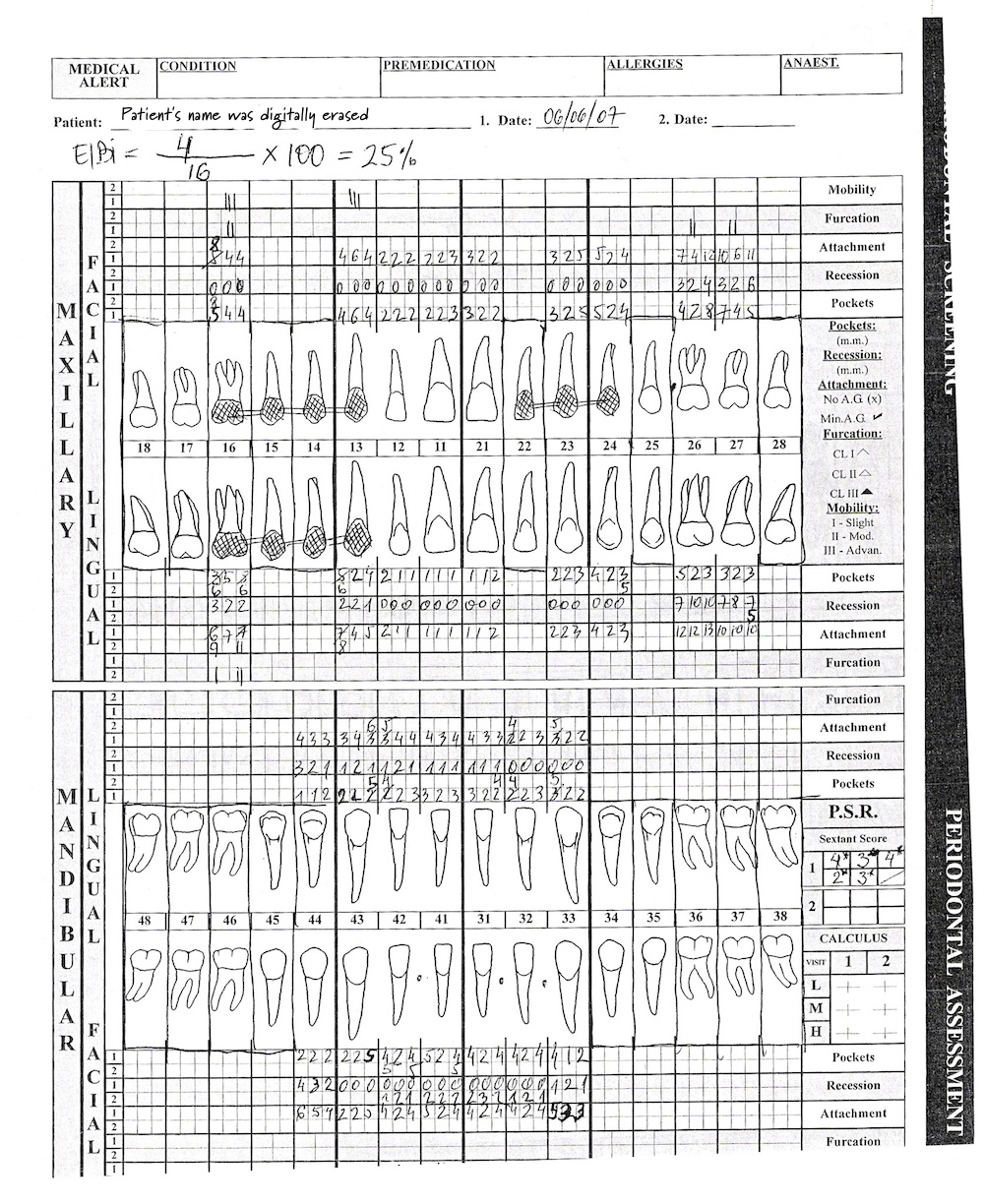
EIBI
EIBI was performed and the result was 25% of bleeding sites. Bleeding on using the stimudent appeared on a mesial of 26 in interproximal spaces of mandibular anterior incisors. There was a greater amount of bleeding on probing that lead me to a conclusion that localized presence of blunt interproximal papillae made EIBI results no quite accurate as they were supposed to bePSR
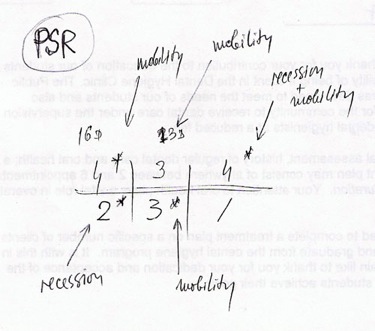
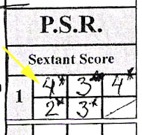
PSR was not measured in sextant 4 due to edentulous area, so I got results only for 5 sextants. Two maxillary posterior sextants had readings of code 4, two anterior sextants had code 3 and sextant 6 had code 2. Five asterixes were noted:
- In sextant one due to the mobility of the bridge
- In sextant two due to a mobility of golden bridge abutment 13
- In sextant three due to a recession of 26 and 27 greater than 3.5mm, and mobility
- In sextant five due to mobility of all lower anterior incisors
- In sextant ix due to a recession of 44 greater than 3.5 mm.
Periodontal Assessment
Due to a presence of accumulation of calculus it was decided to perform periodontal assessment after the debridement of each quadrant respectively.
Periodontal pockets: generalized presence of periodontal pockets of 4 to 8 mm. in posterior segments and 3 to 5 in anterior segments with localized deeper pocketing of 13 ( pockets of 6 mm.)
Recession of 1 to 2 mm. present on lingual of mandibular anteriors, and 4 mm. on distal of 44. The most severe recession was present in 26 and 27 where from buccal a recession of 2 to 6 was noted while on lingual recession was more significant and it ranged between 7 and 10 mm.
Mobility: Class I mobility was present on mandibular lateral incisors and class II on mandibular central incisors. The most significant mobility was noted on the abutments of the golden bridge 13 and 16, where presence of mobility in both horizontal and vertical directions was present and it as classified as Class III.
Furcation involvement: Class I and II was present on all three remnant maxillary molars.
Clinical attachment loss was the greatest in 26 and 27 and it was between 10 and 13 mm.

Nutritional Assessment and analysis
Client was given three day dietary diary to fill out, s I would be able to analyze here dietary habits and give her few suggestions what she is deficient in and what she has a higher intake in her diet.
I asked my client to do diary one day during the weekend and two days during the week.
Using Heath Canada Food Guide I was able to analyze her diet. This was the result:

In my client's diet there was a deficiency in:
- fruits and veggies of 2 servings per day (6 for three days)
- grains of 2 servings per day (6 for three days)
- dairy of 1.5 serving per day ( 5 for three days)
Only overtake of servings was as usual meat and proteins 2.5 servings per day (7.5 for three days).
When my client was scheduled for Oral Hygiene instructions, I explained my client the analysis and stressed out the need to get extra servings of fruits, veggies, grains and especially dairy since my client is in the period of her life when she needs more vitamin D and calcium for her bone mineral density that usually is found in diary.
My client was very impressed of this simple yet very thorough analysis and promised that in near future she will do modifications in her diet so deficient servings will be annulled.
Dental Hygiene Diagnosis
After collecting al the assessment data, I preceded to formulate Dental Hygiene diagnosis for my client.
Four dental hygiene diagnostic statements were made at this time to comprehensively picture client’s oral status:
- Moderate generalized chronic gingivitis with moderate recession in sextants 1 and 5 and severe recession in sextant 3 related to increased accumulation of supra and subgingival soft and hard deposits.
- Moderate generalized chronic periodontitis accompanied with mobility in sextants 1 and 5 and furcation involvement in sextants 1 and 3 related to a generalized early bone loss and localized moderate bone loss in 17,26,27,32 to 42.
- Slightly coated tongue related to inadequate brushing technique
- Increased bleeding and accumulation of supra and subgingival plaque related to ineffective interproximal plaque control.
Planning – RDH Treatment plan
Between to sessions of clinic I developed my Dental hygiene plan for all interventions that will be needed for my client in order to meet her human needs for oral health.
My preliminary plan was use of Local Anesthesia but after the conversation with client and her statement that she wouldn’t like use of local anesthesia because she has lower threshold of pain I have abandon use of LA in a future treatment.
Due to a presence of remnants of a root at 21 I was asked by attending dentist to avoid that area for debridement.
All the rest was pretty much the standard planning of dental hygiene interventions:
- Oral hygiene instructions when I will modify clients brushing technique into Rolling technique and try to convince client to start flossing
- Demonstrate daily tongue brushing in order to decrease plaque accumulation on the tongue
- Periodontal debridement with hand-activated and power-driven instruments to eliminate major and contributory causes of gingival and periodontal inflammation.
- Fluoride treatment with tray method to decrease and arrest caries occurrence
Implementation
Oral Hygiene Instructions
Oral hygiene instructions were given to client prior the beginning of periodontal debridement.
I asked client to modify her brushing technique and to use Rolling stroke technique due to a recession present, I demonstrated use of floss and asked her to consider using floss, at least in occasional basis, and I wrapped up my OHI with demo of tongue brushing and its importance in daily oral self care.
Periodontal debridement
Periodontal debridement was completed in three appointments:
- First appointment: quadrant 1
- Second appointment: quadrants 2 and 3
- Third appointment: quadrant 4
Challenges during the debridement
Periodontal debridement of quadrants 1, 2 and 3 was completed in combination of ultrasonic scaler with hand-activated instruments., while after the completition of quadrant 2 and in second visit, client has developed sensitivity, so when she came for the third visit, I had not to provoke sensitivity and n the same time not to use local anesthesia.. My choice was use of hand-activated instruments exclusively for quadrant 4, thus avoiding sensitivity.
Fluoride treatment
Tray method was chosen for delivery of 2% NaF in foam form. Fluoride present in the clinic required one minute to be applied to take effect.
Evaluation

Outcomes of Dental Hygiene Care
28 days after the second visit client came for evaluation of my implemented dental hygiene treatment. I performed visual evaluation, as well as extra, intraoral exam, gingival evaluation, PSR and complete periodontal evaluation. During this visit I was able to note following changes:
- Client modified her brushing technique into Rolling stroke technique.
- She tried flossing twice and stated that will do it more often
- She cleanses her tongue on a daily basis
- Colour of gingiva at 27 has changed from purple to pink-red
- Sensitivity has occurred due to the removal of calculus and exposure of the roots
- Presence of plaque and calculus was completely eliminated
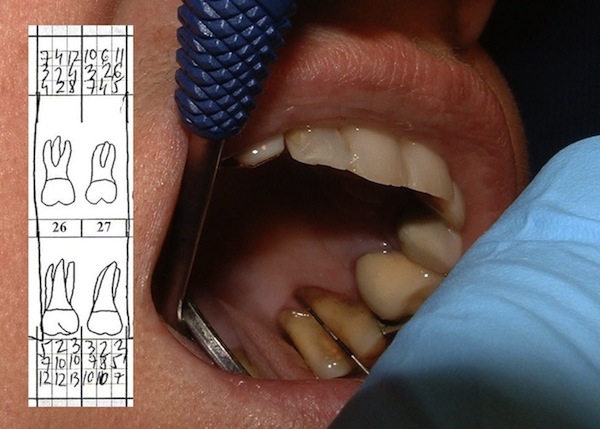
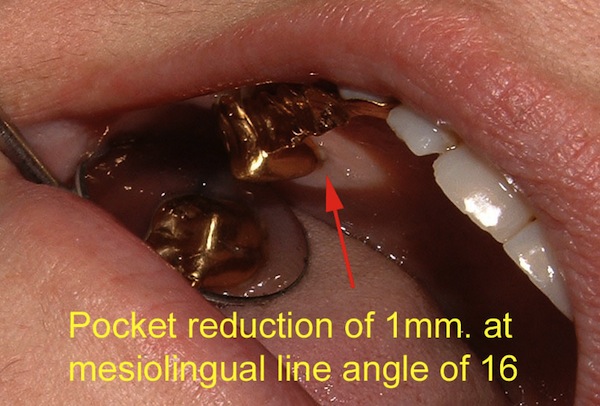
- PSR readings in quadrant 1 has changed from code 4 into code 3 due to a appearance of long junctional epithelium on mesiolingual line angle of 16: CAL readings in the assessment phase were 8 mm. for evaluation day CAL has decreased to 7 mm., pocket depth has decreased from 6 to 5 mm.
 --------
--------
Client was asked in three months to visit her dentist in Macedonia for Supportive periodontal therapy. All of my goals from client’s dental hygiene treatment plan were achieved. Overall this was a beneficial therapy for client and with evaluation healing of the tissue was noted and clients compliance to improve her oral self care maintenance was obvious.
Intraoral images of dentition and supporting oral structures after NSPT


Before and After images



Bibliography
- Darby, M.L and Walsh, M.M; Dental Hygiene Theory and Practice; (2nd.Ed.) 2003
- Department of Nutrition at the Harvard School of Public Health http://www.hsph.harvard.edu/nutritionsource/index.html
- Glycemic index web site; University of Sydney: http://www.glycemicindex.com
- Healthy Fats to Eat As Part of a Nutritious Diet by Anne Collins http://www.annecollins.com/good-fats-to-eat.htm
© January, 2008. All rights reserved.
