SYSTEMIC LUPUS
ERYTHEMATOSUS |
 |
Author:
Dr. Boban Fidanoski, DMD |
| Definition
Systemic Lupus Erythematosus is chronic inflammatory multisystem disease of unknown etiology. It is an autoimmune disease where body’s immune system (antibodies in this case referred to as autoantibodies) mistakenly attacks its own tissues, causing multi-organ inflammation and diverse clinical manifestations with domination of peripheral symmetric polyarthritis of small and large joints. SLE is characterized with periods of exacerbation and remission. Origins of the name: Systemic Lupus Erythematosus “Lupus” is Latin for wolf, “Erythro” in Greek
stands for red, and Systemic is English word meaning that multiple organs
are involved. One theory explains that this disease has gotten its name
because it is similar to the attacks of a wolf on humans with its severity,
random spots of attack and repetitiveness. |
||
 |
||
| Pathogenesis:
SLE results in tissue damage caused by attack of autoantibodies and immune complexes. It involves polyclonal and antigen-specific T and B lymphocyte hyperactivity. T cell help in production of autoantibodies is critical for development of full-blown disease. Proposed Etiology: Definitive etiology is still unknown. We could only hypothesize what causes this disease is: genetics, environmental factors (sun exposure to UV light), estrogen (prepubertal and postmenopausal women have similar incidence to men; men with SLE have higher concentration of estrogenic metabolites), infection (viral: non-specific stimulant of immune response, medications (Dilantin-anticonvulsant), oral contraceptive pills are associated with exacerbation (they should be avoided in SLE patients). 25% of SLE patients have experienced false-positive tests for syphilis due to circulating lupus anticoagulant in the blood. |
||
 |
||
| Differential Diagnosis:
Diagnostic criteria updated by American College of Rheumatology in 1997 states that at least 4 or more of 11 (7 clinical and 4 laboratory) criteria must be present serially or simultaneously: Diagnostic Criteria Description Laboratory tests that will determine diagnosis of Lupus: • Serologic diagnosis made by high titre of ANA detected by immunofluorescence,
but this test doesn’t determine diagnosis because many other autoimmune
disease have positive ANA test
Signs and Symptoms: 1. Musculoskeletal |
||
 |
||
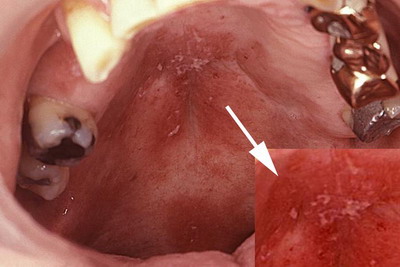
| 3. Oral Painless, shallow oral ulcers, most often occur on the hard and soft palate. There is also a mild involvement of mucosal ulcers as symptom of this disease. Oral ulcers occur at onset in 11% of patients, while at any time are present in 30% of patients. The lesions appear as maculae (red patches) that will later transform into irregular erosions and ulcers which often heal with scarring. Purpuric lesion such as ecchymoses and petechiae may occur. In 30% of the cases, pathology of major salivary glands may occur leading to secondary Sjogren’s syndrome and severe Xerostomia |
||
 |
||
 |
||
 |
||
| 4. Gastrointestinal Renal involvement occurs in about 50% of patients, with only few % with irreversible changes. Proteinuria is the most common clinical sign. Other signs are: Pancreatitis, Lupus Enteropathy, Hepatitis and Hepatomegaly 5. Systemic Fever, Malaise/Fatigue, Lymphadenopathy, Weight loss 6. Cardio-Vascular Pericarditis is the most common cardiac manifestation, occurs up to 30% of patients. Raynaud’s phenomenon, Thrombosis, Vasculitis, Livedo reticularis, Hemolytic anemia (most common vascular manifestation, in almost all patients), Leukopenia (50% of patients), Lymphopenia, Thrombocytopenia. 7. Ophtalmic Conjunctivitis, Episcleritis, Keratokonjuctivitis (occurs in 20% of patients) 8. Pulmonary Interstitial lung disease, Pulmonary hypertension, Alveolar hemorrhage, and Pleuritis. 9. Neurological Depression, Personality disorder, Cerebritis, Transverse myelitis, Seizures, Headache and Peripheral neuropathy First symptoms to occur: 1. Fatigue 2. Myalgias 3. Arthtritis Radiographic characteristics: Radiographically, the arthritis of SLE is non-erosive. This is helpful
for differential diagnosis with Rheumatoid Arthritis where there is
bone erosion on radiographs. |
||
 |
||
| Microscopic features / histoanalysis:
Three histological lesions are most characteristic of SLE: Microscopic features of oral lesions: Histologically, lesions reveal lichenoid mucositis with perivascular exudate and thickening of basement membrane. Demographics/Epidemiology: Prevalence: 0.05%, 15 to 50 per 100,000 population
in USA. Treatment: Systemic Lupus Erythematosus is a disease without
a known cure, so treatment is based on relieving symptoms, suppressing
inflammation, and preventing future pathology. Symptomatic treatment
is tailored for the organ involved and for severity of the disease:
use of topical sunscreen, avoid UV light and estrogens, use of NSAID’s
for arthritis, use of antimalarials for dermatologic manifestations,
use of topical steroids for rash, use of systemic steroids for prevention
of end organ damage. Calcium and Vitamin D to fight osteoporosis, use
of Corticosteroids as immunosuppressant drugs for serious organ involvement
(e.g. Cerebritis, nephritis). All medications used to treat SLE require
periodic monitoring for potential toxicities. |
||
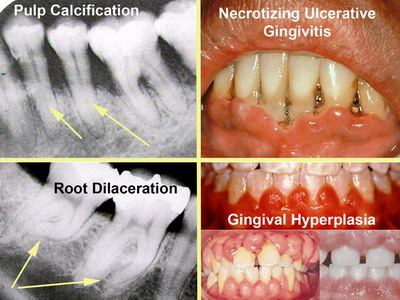
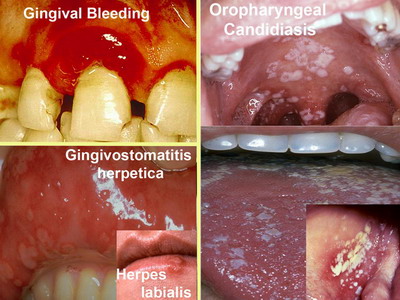
| Adverse effects of Lupus therapy in oral
cavity:
Long term use of medications to control Lupus can induce significant
intra-oral pathology. |
||
 |
||
 |
||
| Treatment of adverse effects of Lupus
therapy in oral cavity :
Preventive dental hygiene care in Lupus patients is very important.
Chlorhexidine mouthwashes could help contain periodontal disease. Mucous
membrane ulcers can be treated with hydrogen peroxide gargle, buttermilk
gargle, or steroid impregnated gel. Intralesional injection of corticosteroids
are also effective. Bacterial, viral and fungal infection should be
treated with conventional, proven therapy specific for the infection
present. Dental procedures should not be undertaken on patients with
active Lupus, or if necessary, antibiotic premedication is advised,
due to high incidence of bacterial endocarditis. |
||
 |
||
| Lupus prophylaxis before dental hygiene
treatment: Lupus is considered as high-risk category of disease by The American National Guideline Clearinghouse and American Academy of Dermatology so they recommend that patients with this kind of condition require antibiotic premedication before dental treatment. |
||
 |
||
| Prognosis:
Survival in patients with SLE is 90 to 95% at 2 years, 82 to 90% at 5 years, 71 to 80% at 10 years, and 63 to 75% at 20 years. Disability in SLE patients is common. 20% of patients experience remissions. Infections due to immunosuppressive therapy and renal failure are the leading causes of death in the first decade of disease. Thromboembolic events are frequent causes of death in the second decade.
Quotes about Lupus: "Homo homini Lupus est."
– Plautus, year 254 before Christ. (Latin phrase meaning: Man
is a wolf to his fellow-man) ______________________________________________________________________
Written literature: Andreoli, T.E. et al. (1997): Cecil Essentials
of Medicine; (4-th ed.)-W.B.Saunders Company,U.S.A. Internet resources: Long, R.G. et al. (1998): Oral manifestations
of systemic diseases, The Mount Sinai Journal of Medicine(N.Y.-USA)
Vol. 65, No.5-6 Photographs: http://www.merckmedicus.com/ppdocs/us/hcp/content/white/chapters/white-ch-010-s002.htm |
||
author: Boban Fidanoski; researched for the purposes of the studies at the CCDH
and published on-line in July-August 2007 |
||
 |

